In This Issue...
Jeff Weighs In
MCRs in the Community
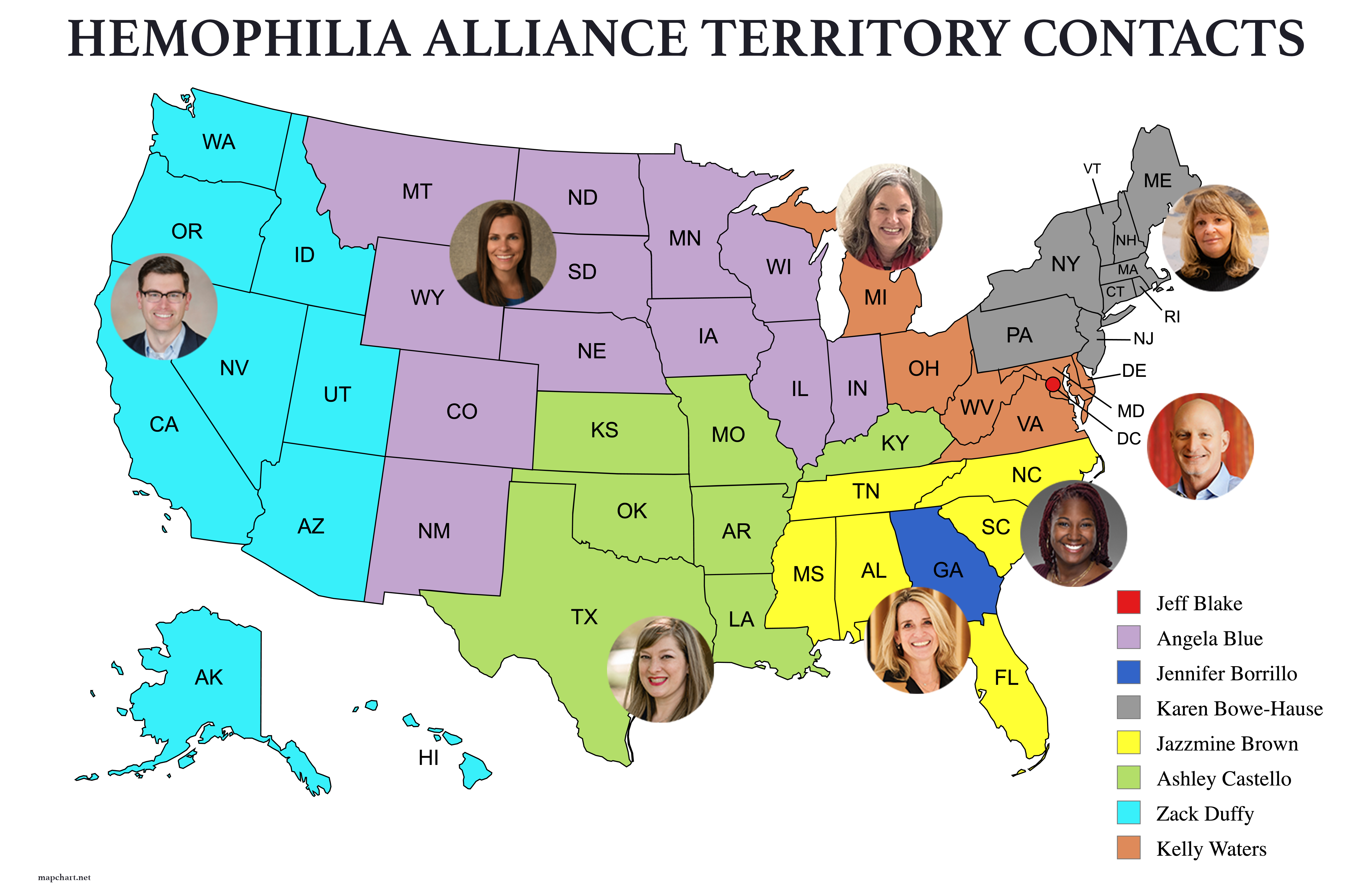
Announcing New MCR Territory Coverage Assignments
by Jennifer Borrillo, Senior Vice President Member & Community Relations
Ashley Castello, Jazzmine Brown, and Kelly Waters joined the Hemophilia Alliance team in September as new Directors of Member & Community Relations. These new additions reflect both expansion and transition within the team—one new position, one to succeed Jeff Amond, who recently left the Alliance, and one to follow Mark Plencner, who will be retiring in January of 2026.
At the Fall Member Meeting held in Washington, DC on September 6, 2025, the updated MCR Territory Map was shared with attendees and those in attendance were able to meet Ashley, Jazzmine, and Kelly in person. The entire Hemophilia Alliance team, and the MCRs in particular have worked so closely with our member HTCs, and are sensitive to the uncertainty change brings, no matter how exciting it can be. Angie, Mark, Karen, Zack, and Jennifer will still be working with each of their previously assigned HTCs throughout the remainder of 2025, while also personally introducing Ashley, Jazzmine, and Kelly to the HTCs they will become the primary MCR contact for in 2026.
Your primary MCR is your first point of contact for Hemophilia Alliance communications. Your assigned primary MCR contact will triage your questions and issues, help assess next steps, assist with strategic discussions, and help with planning for the future. The MCRs are a small but mighty team that quickly pulls in other team members to provide guidance and/or to resolve issues as needed. Remember to notify your MCR contact as soon as you have a question or an issue arises. Reaching out to the MCR team proactively allows for early intervention and helps the MCR team to better address issues in a timely manner. If you are running into an issue, it is likely that another HTC is running into a similar issue.
We cannot stress enough that there are no “stupid” questions, so please reach out to your primary HTC MCR contact with any questions you may have. We are here to help you navigate those questions and find the answers, viable solutions, and resources needed. Remember, we work for you!
| Name | Phone | |
|---|---|---|
| Jennifer Borrillo, MSW, LCSW, MBA | borrillo@hemoalliance.org | 504-376-5282 |
| Angela Blue, MBA | angela@hemoalliance.org | 651-308-3902 |
| Karen Bowe-Hause, MBA, MT | karen@hemoalliance.org | 717-571-0266 |
| Zack Duffy, MBA | zack@hemoalliance.org | 503-804-2581 |
| Mark Plencner | mark@hemoalliance.org | 701-318-2910 |
| Ashley Castello, M.Ed. | ashley@hemoalliance.org | 225-266-5062 |
| Jazzmine Brown, MBA, MSW, LCSW | jazzmine@hemoalliance.org | 770-570-2649 |
| Kelly Waters, MSW. LCSW | kelly@hemoalliance.org | 804-317-4998 |
| Kollet Koulianos, MBA | kollet@hemoalliance.org | 309-397-8431 |
| Roland P. Lamy, Jr. | roland@hemoalliance.org | 603-491-0853 |
| Dr. George L. Oestreich, Pharm.D., MPA | george@hemoalliance.org | 573-230-7075 |
Building Connections and Navigating Change in Medicaid Leadership
by George Oestreich, Government Payer Consultant Hemophilia Alliance
Staying connected with your state Medicaid leadership is more important than ever. For Hemophilia Treatment Centers (HTCs), building relationships with your state’s Medicaid director and pharmacy program staff can make a real difference in shaping policies and reimbursement processes that affect patient care. Recent discussions among the National Association of Medicaid Directors Alumni Group have highlighted new challenges and opportunities, especially as Medicaid program leadership changes continue across the country.
Who’s New? Medicaid Director Transitions
There’s been a wave of new appointments and interim directors in Medicaid programs nationwide. Here are some of the latest changes:
- Idaho: Sasha O’Connell is now leading, succeeding Juliet Charron.
- Illinois: Laura Phelan has taken over from Kelly Cunningham.
- Wyoming: Jesse Springer is serving as interim director, following Lee Grossman.
- Iowa: Lee Grossman is now director, succeeding interim Rebecca Curtis.
- Louisiana: Drew Maranto is interim director, succeeding Kim Sullivan.
- Maryland: Perrie Briskin has replaced Ryan Moran.
- Nevada: Ann Jensen is now director, succeeding Stacie Weeks.
- Vermont: Ashley Berliner is interim director, following Jill Olson.
- Utah: Nate Checketts is interim director, succeeding Jen Strohecker.
- Puerto Rico: Luz Cruz is interim director, succeeding Carlos Santiago-Rosario.
- Ohio, Missouri, New Mexico: New directors are yet to be determined.
These transitions mean that many states are adjusting to new leadership styles and priorities. For those working with Medicaid, it’s a good time to review your contacts and consider reaching out to introduce yourself or reconnect.
Facing Today’s Challenges
Medicaid directors are dealing with tough challenges, including budget constraints and operational disruptions. Reduced federal revenue and the lack of reserve accounts in some states are putting extra pressure on agencies. Many directors are navigating budget downturns for the first time, making peer support and shared best practices more valuable than ever. Without HTC input, the agencies will not know how the new landscape will impact your ability to efficiently manage your patient’s bleeding disorders, which are known to be expensive to treat.
In summary: The landscape of Medicaid leadership is changing rapidly, and HTCs, who work with Medicaid programs, can play a vital role by building relationships, offering support, and staying informed about new developments. It is imperative for you to help your state’s Medicaid program understand how these changes can help you better serve Medicaid-eligible patients and contribute to positive value-added outcomes.
Open Enrollment is Upon Us: BEWARE OF JUNK HEALTHPLANS
by Kollet Koulianos, Senior Payer Consultant Hemophilia Alliance
As healthcare open enrollment nears, it’s essential for our HTCs to inform patients who are buying their own insurance (outside of employer-sponsored plans) about the dangers of “junk health plans.” These plans often provide limited coverage and can leave patients with significant out-of-pocket costs. Junk plans are expected to be more common this year, except in the 12 states and Washington, D.C., that have passed laws banning their sale. However, even in those states, certain junk plains (such as Christian ministry plans and Farm Bureau plans) are still allowed to be sold. These plans aren’t classified as insurance but often function as what we consider “junk plans,” especially for those with chronic health conditions.
These plans are often appealing because of their affordability but come with major red flags: limited provider networks, no prescription drug coverage, and exclusions for pre-existing conditions or high-cost specialty medications. For people living with diseases like hemophilia, multiple sclerosis, diabetes, or cancer, those gaps aren’t just inconveniences—they’re life-threatening.
Chronic disease care requires consistency, coordination, and access—not fine print. Before enrolling, patients should verify that a plan covers their prescribed medications, make sure their specialists are in-network, and the plan complies with Affordable Care Act protections.
How Our Patients Can Identify Junk Health Plans
1. Look for the Fine Print
If a plan doesn’t comply with Affordable Care Act (ACA) requirements—such as covering essential benefits—it’s not true comprehensive insurance. Signs might include:
- Excluding preexisting conditions or limiting annual payouts.
- Not covering specialty medications
- Being described as “temporary,” a “bridge plan,” “health sharing,” or “fixed indemnity”
- Capping coverage, requiring large upfront payments, or refusing to cover your medications of specialists
- Make sure your specialist and/or treatment center is actually in network. Some junk plans claim you can “see any doctor,” but offer little to no reimbursement for those visits
2. Red Flags to Watch For
Be cautious if a plan shows any of these warning signs:
- Not available on Healthcare.gov
- Marketed through social media ads or robocalls
- Sold by “benefit associations” or “faith-based” groups rather than licensed insurers
For chronic conditions, prescription coverage is crucial, watch for:
- “Discount cards” instead of real prescription coverage
- Exclusion of specialty medication
- Use of “alternative funding” schemes that require you to apply for copay assistance instead of using your insurance benefits
Remember: Only ACA-compliant plans sold through legitimate state or federal marketplaces guarantee essential health benefits and consumer protection.
3. Trust Your Instincts
If the deal seems too good to be true (such as $200/month for “comprehensive” coverage) it almost always is.
Bottom Line
Real health plans protect you when you need care the most. Junk plans protect insurers’ profits instead. Before enrolling, check with:
- Healthcare.gov
- Your state insurance department
- Reach out to your MCR team member at the Hemophilia Alliance.
Because when it comes to chronic disease, a “cheap” plan can become the most expensive decision of your life.
Washington Update
Advocacy and Legal Team – Legislative and Regulatory Updates
by Artemis Policy Group
Government Shutdown Begins – and Continues
Congress was unable to pass legislation to fund the government before fiscal year 2026 started on October 1st. As a result, the federal government has been shut down: “essential” personnel are working, while other federal staff are furloughed. The shutdown is now the longest full shutdown on record.
Selected federal programs – and how they are impacted by a government shutdown | |
Social Security | Benefits continue. Social Security is considered a mandatory program; funding and Social Security payments are not interrupted. |
Medicare | Benefits continue. There may be interruptions to some incidental services, e.g., issuance of replacement Medicare cards.
|
Medicaid | Benefits continue. According to the US Centers for Medicare and Medicaid Services, the federal government has enough money to fund Medicaid for the first quarter of fiscal 2026. |
Supplemental Nutrition Assistance Program (SNAP) | The US Department of Agriculture has announced that it will not tap its $5 billion contingency fund to maintain SNAP benefits. Many states warn they will be forced to suspend SNAP benefits by November 1. |
Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) | Benefits continue for now, based on a temporary funding workaround announced by the White House, but some states warn they may run out of funding as soon as November 1. |
Head Start | Programs continue for now, though disruptions are possible later in the year. |
US Postal Service | Post offices will be open as usual and USPS will continue to deliver mail. |
It is unclear when the shutdown stalemate will be resolved. The House has not met in session since it passed a stopgap funding bill and left town on September 19th. The Senate, for its part, continues without success to hold votes on the House-passed bill. Republicans are seeking to pass a clean temporary funding measure (“continuing resolution” or CR), while Democrats are insisting that Congress act to extend the expiring enhanced Affordable Care Act (ACA) premium subsidies.
Alliance Hill Day
Despite the government shutdown, the Alliance was able to hold its biggest ever Hill Day on October 7th. Over 130 participants (including 24 patients) attended 10 member-level meetings with Senators or Representatives, and 111 meetings with Hill staff; they also made dozens of unscheduled drop-in visits to leave behind Alliance materials. Participants described the integrated, comprehensive care that HTCs provide; the importance of the 340B Program to the national network of HTCs; the vital role played by federal health programs at CDC and HRSA in supporting HTCs and HTC patients; and the affordability and access challenges that currently impact patients with bleeding disorders across the country.
340B Legislation and Hearing
Representative Buddy Carter introduced H.R. 5256, the 340B ACCESS Act, on September 10th. This bill raises the same concerns as last year’s almost identical legislation, such as a restrictive patient definition, burdensome transparency requirements, and constraints on subgrantee participation in the 340B program. Alliance Hill Day participants addressed many of these topics during their meetings, and the Alliance policy team will continue to monitor this bill along with any other 340B reform efforts.
On October 23rd, the Senate Committee on Health, Education, Labor and Pensions (HELP) held a hearing on The 340B Program: Examining Its Growth and Impact on Patients. The committee heard from Michelle Rosenberg (U.S. Government Accountability Office), Aditi Sen (Congressional Budget Office), and Dr. William Feldman (UCLA). The focus of the hearing was on the September 2025 report from the Congressional Budget Office on Growth in the 340B Drug Pricing Program and past analysis by the GAO and research on 340B by Dr Feldman and colleagues. There was good attendance at the hearing, and most Senators expressed support for the 340B program, especially those from more rural states There was also bi-partisan support for greater oversight by the Office of Pharmacy Affairs and covered entity reporting on revenue and how funds are used.
Administration and Operations Update
No Tricks, Just Impact: Fall Meeting Highlights
Happy Halloween from all of us! We hope your day is filled with treats, laughter, and a little bit of spooky fun.
The Fall Member Meeting and Hill Day, hosted on October 5-7th, were both very well attended and highly productive. This year, we introduced a new meeting schedule. The shift to a one-day meeting format followed by Hill Day was widely appreciated. Members found the condensed schedule to be both manageable and meaningful, allowing them to stay connected without extended time away from their Hemophilia Treatment Centers.
One of the most appreciated aspects of the Member meeting continues to be Alliance “updates” – Washington, Compliance, Medicaid and Payer – which provided timely insights into what is going on in D.C. regarding Medicaid developments and payer issues. These sessions were described as “essential” and “eye-opening,” helping members stay informed and empowered. One first time attendee commented “…90% of the content of this meeting was relevant to my position at my HTC.”
Equally valued was the chance to network and collaborate. The meeting served as a vibrant hub for professionals across the country to share experiences, challenges, and solutions. As one attendee put it: “It was so good to reconnect with colleagues from across the country. The energy in the room was palpable, and the sessions were both informative and inspiring.”
The diversity and clarity of presentations also stood out. Members appreciated the range of topics and the engaging delivery. We did hear a call for speed networking and breakout discussions in future events.
Despite the government shutdown, members made the most of Hill Day, spending a productive afternoon educating legislators about hemophilia, the Hemophilia Alliance’s 340B program (HM 340B), and the critical importance of comprehensive services. The commitment to advocacy and awareness was evident, reinforcing the community’s dedication to improving care and support nationwide. Hop on over to the Advocacy and Legal Team section of the newsletter for more details on our day on the Hill.
Finally – We get a lot of questions about our member meetings – specifically, what is the purpose and how are they funded? Hemophilia Alliance hosts 8 in-person meetings, 4 of which offer CEUs. Alliance meetings are a member benefit. All member meetings aim to provide opportunities to network and share best practices. Please visit our Member Meeting FAQs page on our website for additional information. And as always, feel free to reach out to Theresa Parker, Manager of Meetings and Events, with questions.
To see our meeting calendar for 2026 – click on our downloadable 2026 Alliance Meeting Calendar – all dates are final except for a small adjustment to our 2026 Fall Member Meeting and Hill Day in Washington, DC – we are working to get that confirmed to take place in September 2026.
{kind=link}
2026 MEETINGS | DATE |
|---|---|
Medical Providers & Business Administrators Meeting [APPLICATION CLOSED] | January 11th – 13th, 2026 (Newport Beach, CA) |
Pharmacists CE Meeting [APPLICATION CLOSED] | January 21st – 23rd, 2026 (Tampa, FL) |
Linda Gammage Social Workers CE Meeting [APPLICATION OPEN NOV. 6 – 20, 2025] | February 25th – 27th, 2026 (Oklahoma City, OK) |
Spring Members Meeting [SAVE THE DATE] | March 8th – 10th, 2026 (Seattle, WA) |
New HTC Staff Meeting [SAVE THE DATE] | April 21st – 23rd, 2026 (Aurora, CO) |
Nurses CE Meeting [SAVE THE DATE] | May 3rd – 5th, 2026 (Chicago, IL) |
Physical Therapists CE Meeting [SAVE THE DATE] | May 6th – 8th, 2026 (Chicago, IL) |
Fall Members Meeting & Hill Day [SAVE THE DATE] | TBD (Washington, DC) |

We’d love your input on future newsletter topics