
5th Annual Pharmacist CE Meeting – The Best Yet!
by The MCR Team

[Click on image for larger version]
The Hemophilia Alliance 5th Annual Pharmacist CE Meeting was held January 21-23 in Tampa, Florida at the Current Hotel. In attendance were 54 pharmacists in-person and another 32 pharmacists and pharmacy technicians joining virtually. The faculty was outstanding, with attendees reporting “this may have been the best conference yet”!
Thank you to Takeda and The Alliance Pharmacy (TAP) for sponsoring this event. Takeda and TAP have sponsored every Pharmacist CE meeting for the last 5 years! Thank you, too, to the Indiana Pharmacy Association for reviewing 12 faculty presentations which can be submitted for ACPE credits for the next three years. This brings the total to 36 active CE credits available for home study for pharmacists and technicians. A grand total of 62 CE credits have been provided over the last 5 years. This is a marvelous benefit that is exclusive to our Hemophilia Alliance members.
The Pharmacists CE Planning Committee worked diligently to build another strong program. With the pending retirement of Mark Plencner, Heidi Lane, Angie Blue, and Theresa Parker joined veteran committee members Angela Kellum, Dana Smith, Stevan Mizimakoski, Matt Debrine, and Mark. The team worked hard to pull the program together in record time.
Topics covered during the conference included: sickle cell disease, AI in the pharmacy, patient assistance programs, von Willebrand disease diagnosis and therapies, inhibitors, new and emerging therapies in hemophilia, physical therapist-pharmacist collaboration, reproductive health for women with bleeding disorders, and autoimmune hematology.
Thursday’s dinner at the Rusty Pelican included a nice tribute to retiring Mark Plencner from both Jeff Blake and Stevan Mizimakoski which included a video presentation highlighting family and HA team activities.

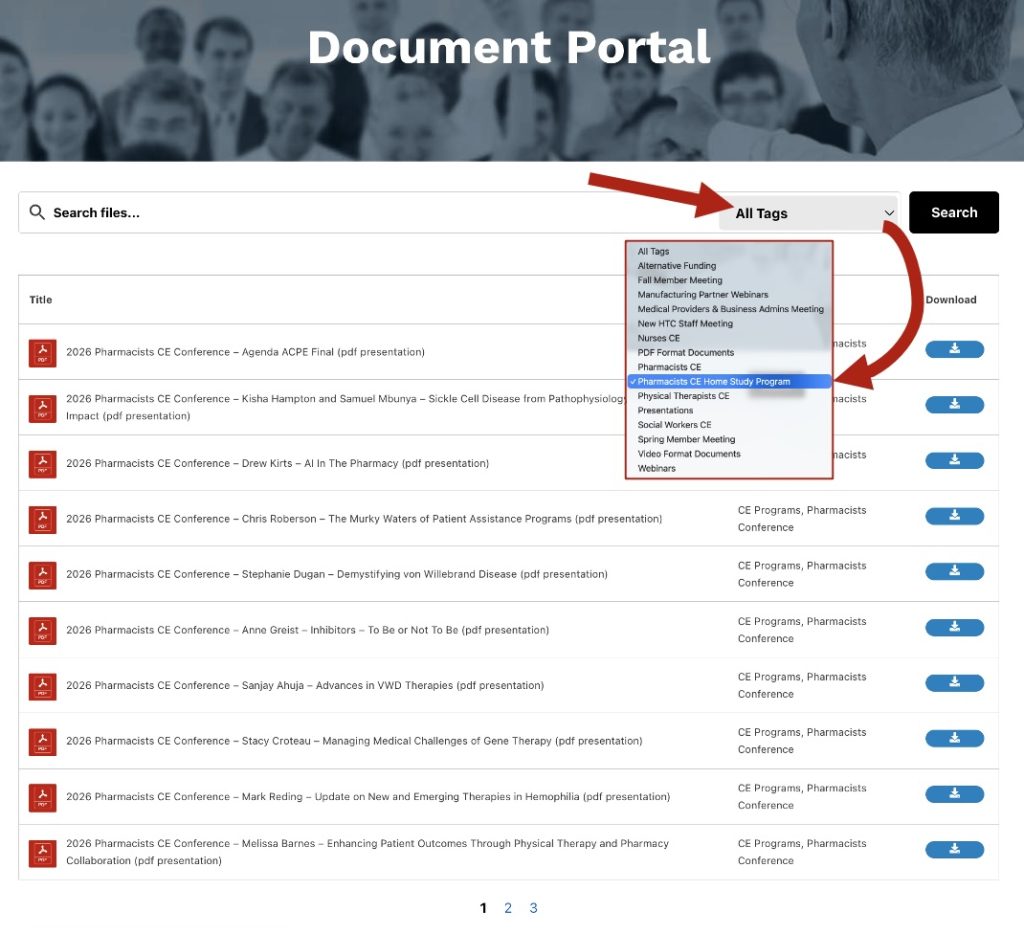
All the substantive video presentations from this meeting are posted on the Hemophilia Alliance website in the document portal. Do yourself a favor and view the presentations. It will be well worth your effort. You will be impressed with the knowledge and expertise that is shared by members of our HTC community.
Information for submitting CE credits for home study is available on the Hemophilia Alliance website under the Document Portal section. Please note a login is required. If you are a member HTC of Hemophilia Alliance but don’t have a login, click here to request for one.
Program development is underway for 2027. Save the date: February 24-26, 2027. We look forward to seeing you then!
MPBA 2026 Meeting Recap: Strengthening the Future of HTCs Through Leadership, Strategy, and Collaboration
by The Admin & Ops Team
The Hemophilia Alliance kicked off the year with the Medical Provider & Business Administrator (MPBA) Meeting, held January 11–13 in Newport Beach, CA. Member HTC clinical and business leaders from across the country gathered for this Alliance-funded program to strengthen leadership, improve operations, and foster collaboration.

[Click on image for larger version]
The program opened with an optional pre-conference featuring a foundational session on HTC and 340B essentials, paired with a more advanced topic highlighting the gold standard for HTC–pharmacy integration, Building an Inhouse Pharmacy, before participants transitioned into the main agenda.
Program Highlights and Participant Feedback
Day 1
- HTC Models & Innovation: A valuable look at the range of center types and creative approaches to care delivery.
- Patient Support Services: Meaningful insights on documentation, compliance, and patient centered service models.
- Leadership Essentials: Invited speaker, Paula Mulford, delivered a well-received session outlining practical, memorable leadership strategies that could be implemented immediately.
- Staffing Strategies: Benchmarking across HTCs helped teams identify workforce needs and new approaches for growth.
- Payer & Pharmacy Challenges: This session’s thoughtful facilitation made a complex topic more approachable and validated shared challenges.
Day 2
- Washington Updates: Praised for clear summaries and forward-looking insights about the current policy landscape.
- Novel Therapies: Really valuable, appreciated the perspectives and identified areas for follow up.
- Advocacy: Attendees reported a stronger sense of what they can do locally and how to involve patients in advocacy efforts.
- Strategic Planning Tools: The business plan manual and exercises helped teams begin hands on planning during the session.
Many participants left with concrete next steps, including focusing on their HTC strategic/business plan, seeking more structured feedback from their teams, creating executive summaries/elevator pitches, and strengthening collaboration with local chapters on patient support initiatives.
“The MPBA Meeting has become one of the most valuable gatherings I attend each year. The depth of discussion, practical strategies, and open collaboration help me return to my HTC with fresh ideas and a clearer path forward.” — MPBA Past Attendee
As participation grows each year, it is increasingly clear that the MPBA Meeting is becoming an essential activity for every member HTC, offering unmatched opportunities for learning, strategy, and collaboration.
Save the Date – MPBA 2027: January 24–26
We look forward to bringing the community together again next year!
Notes From The Community
In Tribute to Dr. Lynn Malec
 We are saddened by the passing of Dr. Lynn Malec, a respected hematologist, valued contributor to the bleeding disorders community, and an avid supporter of the Hemophilia Alliance.
We are saddened by the passing of Dr. Lynn Malec, a respected hematologist, valued contributor to the bleeding disorders community, and an avid supporter of the Hemophilia Alliance.
Dr. Malec was an extraordinary physician, researcher, and advocate whose impact reached far beyond her professional accomplishments. She dedicated her life to improving care, advancing access to care, and centering the voices of patients and families. Those who had the privilege of working alongside Lynn knew her as a brilliant clinician, a generous mentor, and a compassionate leader who brought both rigor and humanity to everything she did. Her influence will live on through the countless lives she touched, the colleagues she inspired, and the community she helped strengthen.
Our hearts are with Dr. Malec’s family, friends, colleagues, and the many communities she served. We honor her legacy by reaffirming our commitment to the work she championed—advancing access to care, improving care, and ensuring that patients and families remain at the center of everything we do.
Tool for Pharmacies
by Angela Kellum, PharmD., Louisiana Center for Bleeding & Clotting Disorders
One step in our pharmacy workflow when dispensing clotting factor is determining which vial sizes to combine to meet a patient’s prescribed dose.
Background
Clotting factor products are unique in that the actual unit amount in each vial does not match the unit amount associated with the NDC. For example, a 4,000 unit vial may contain hundreds of units more or less than 4,000. Additionally, many patients require more than one vial per dose due to available vial sizes and individualized dosing parameters.
Importance
Pharmacies calculate vial combinations that meet the prescribed dose while staying within allowable deviation ranges. This matters not only clinically, but also financially. Factor costs are per unit, and cost containment is critical. Also, many pharmacies must comply with strict payor contract requirements, often within very tight ± percentage limits.
We also are mindful of patient convenience and possible adherence challenges and therefore want to minimize the number of vials that patients must store, reconstitute, draw up and infuse. This is especially important for pediatric patients and for those with fragile veins who may struggle with larger infusion volumes.
Challenge
Traditionally we relied on pen, paper, and a calculator. With so many possible vial combinations, this process was slow and often left us wondering whether we truly had found the best option.
Solution
One day while I was working remotely, I asked my son, Samuel—who happens to be very good at math—to help me figure out the optimal vial combination for a patient’s order. He found the answer quickly. Then, later he developed a program that could do the calculation for me! That program can now be found at: https://vialcalculator.com/.
We now use this program almost every day in our in-house 340B pharmacy. I also rely on it when placing large monthly replenishment orders for our contract pharmacy. It has been shared with HTC pharmacy colleagues and hospitals across the state and across the country, and the reaction is always the same—relief that manual calculations are no longer necessary!
How it works
The program is housed on its own website: https://vialcalculator.com/
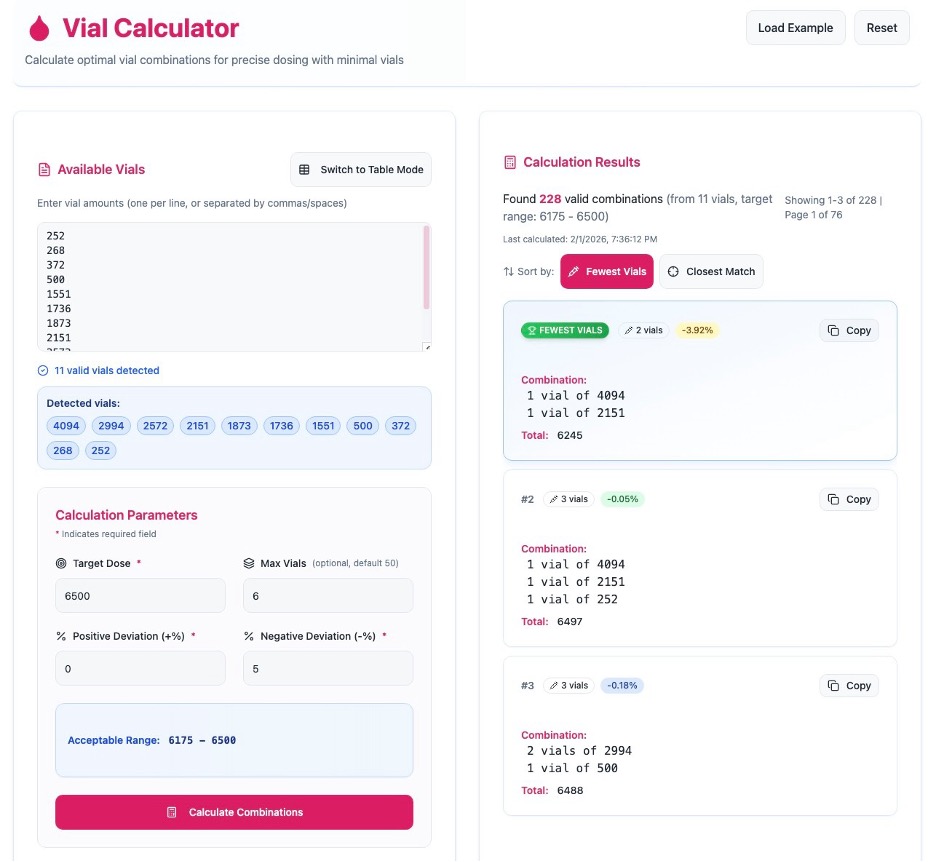
Using the program takes just 3 simple steps:
- Enter vial inventory
Free-type or copy and paste available vial inventory directly into the program—there is no need to remove alpha characters or clean up cells. If inventory is limited for specific vial sizes, “Switch to Text Mode” allows entry of exact vial counts. - Enter dosing parameters
Input the prescribed dose and allowable percent deviation (such as ±10% or +0/−5%). An optional field allows you to set a maximum number of vials per dose or dispensation. The calculator can accommodate up to 100 vials, which is especially helpful for large replenishment orders. - Calculate combinations
With one click, the program instantly generates optimal vial combinations.- Results can be sorted by Fewest Vials or Optimal Combinations
- The selected combination can be copied directly into an ordering email, printed for inventory pulling, or saved for documentation
Final thoughts
This tool has become an integral part of our pharmacy workflow, and it has improved efficiency, confidence, and consistency in factor dispensing. I encourage you to share it with your pharmacy teams and contract pharmacies. I’m confident they’ll find it just as helpful.
For feedback or suggestions, feel free to email Angela Kellum at: akellum1@tulane.edu.